
Leave a message
If you are interested in our products and want to know more details, please leave a message here, we will reply you as soon as we can.







The Clavicle Hook Locking Plate is designed for distal clavicle fractures with AC joint dislocation, offering both rigid fixation and dynamic stability through its unique hook-and-plate design.
Item No :
GOHE087MOQ :
10 PiecesClassification :
Class IIIColor :
No Color/Custom ColorOrigin :
Xiamen, ChinaPayment :
T/T 50% and balance before shipmentLead Time :
Depends on the order circumstancesMedical Titanium Clavicle Hook Locking Plate
Our Clavicle Hook Locking Plate is meticulously engineered for complex distal clavicle fractures with acromioclavicular (AC) joint dislocation. Constructed from high-strength medical titanium alloy, it offers outstanding biocompatibility and fatigue resistance, capable of withstanding the stresses of early shoulder mobilization.
The core of its design is the integrated hook-and-plate construct. The proximal plate section provides rigid fixation to the clavicle via multi-hole locking screw technology, creating an angle-stable frame. The distal hook is inserted beneath the acromion during surgery, leveraging the scapula for mechanical support to provide continuous, stable resistance against superior displacement of the dislocated clavicle, ensuring anatomical reduction and a reliable healing environment.
The plate is pre-contoured to better match the distal clavicular anatomy, reducing intraoperative modification. The low-profile design effectively minimizes soft tissue irritation and the prominence of the implant.
Compatible Screws & Indications:
- Fitted Screw:Ф3.5 Locking Screws, Ф3.5 Cortical Screws;
- Scope of Application: Distal clavicle fractures (Neer Type II), Acromioclavicular joint dislocation (Rockwood III-V).
Specifications of Clavicle Hook Locking Plate:
| Product Code | ITEM | Model | Spec (Holes/Length) |
Material | Left/Right | Product Picture |
| 20351005 | Clavicular Hook Locking Plate-I 15mm | YSA44-01 | Left 5 Holes | A | Left/Right |  |
| 20351006 | Left 6 Holes | |||||
| 20351007 | Left 7 Holes | |||||
| 20351008 | Left 8 Holes | |||||
| 20352005 | Right 5 Holes | |||||
| 20352006 | Right 6 Holes | |||||
| 20352007 | Right 7 Holes | |||||
| 20352008 | Right 8 Holes | |||||
| 20361005 | Clavicular Hook Locking Plate-I 18mm | YSA44-02 | Left 5 Holes | A | Left/Right |  |
| 20361006 | Left 6 Holes | |||||
| 20361007 | Left 7 Holes | |||||
| 20361008 | Left 8 Holes | |||||
| 20362005 | Right 5 Holes | |||||
| 20362006 | Right 6 Holes | |||||
| 20362007 | Right 7 Holes | |||||
| 20362008 | Right 8 Holes | |||||
| 20961004 | Clavicular Hook Locking Plate-I | YSB44-01 | Left 4 Holes | A | Left/Right |  |
| 20961005 | Left 5 Holes | |||||
| 20961006 | Left 6 Holes | |||||
| 20961007 | Left 7 Holes | |||||
| 20962004 | Right 4 Holes | |||||
| 20962005 | Right 5 Holes | |||||
| 20962006 | Right 6 Holes | |||||
| 20962007 | Right 7 Holes | |||||
| 20971004 | Clavicular Hook Locking Plate-I | YSB44-02 | Left 4 Holes | A | Left/Right |  |
| 20971005 | Left 5 Holes | |||||
| 20971006 | Left 6 Holes | |||||
| 20971007 | Left 7 Holes | |||||
| 20972004 | Right 4 Holes | |||||
| 20972005 | Right 5 Holes | |||||
| 20972006 | Right 6 Holes | |||||
| 20972007 | Right 7 Holes | |||||
| 10241005 | Clavicle Hook Plate-Ⅰ(15mm) | YSZQ01 | Left 5 Holes | A | Left/Right |  |
| 10241006 | Left 6 Holes | |||||
| 10241007 | Left 7 Holes | |||||
| 10241008 | Left 8 Holes | |||||
| 10242005 | Right 5 Holes | |||||
| 10242006 | Right 6 Holes | |||||
| 10242007 | Right 7 Holes | |||||
| 10242008 | Right 8 Holes | |||||
| 10251005 | Clavicle Hook Plate-Ⅰ(18mm) | YSZZ01 | Left 5 Holes | A | Left/Right |  |
| 10251006 | Left 6 Holes | |||||
| 10251007 | Left 7 Holes | |||||
| 10251008 | Left 8 Holes | |||||
| 10252005 | Right 5 Holes | |||||
| 10252006 | Right 6 Holes | |||||
| 10252007 | Right 7 Holes | |||||
| 10252008 | Right 8 Holes |
FAQ:
Q1: What is the primary use of the hook plate, and how does it differ from a standard clavicle plate?
A1: It is specifically designed for certain fractures at the very outer end (distal) of the clavicle, often involving dislocation of the AC joint due to ligament rupture. Standard straight or anatomical clavicle plates struggle to control the upward displacement in this area. The key differentiator is the hook itself, which engages under the acromion to "support" and stabilize the dislocated clavicle from below – this is its core advantage.
Q2: Could the hook part irritate or damage structures under the acromion, like the rotator cuff?
A2: A skilled orthopedic surgeon will place the hook in a safe zone beneath the acromion using precise technique to avoid direct impingement on critical structures like the rotator cuff tendons. However, some patients may experience mild sensation of the hook or slight motion limitation during shoulder movement, which is often temporary. This is also the primary reason why a second surgery to remove the implant is commonly recommended after fracture healing (around 6-12 months).
Q3: What are the key rehabilitation considerations post-surgery? When can I start moving?
A3: It is crucial to strictly follow your surgeon's specific protocol. Generally, the arm is protected in a sling initially, but motion of the hand, wrist, elbow, and gentle pendulum exercises for the shoulder are encouraged to prevent stiffness. Around 6 weeks, depending on healing seen on X-ray, more active shoulder rehabilitation typically begins. Activities involving heavy lifting or strenuous motion should be avoided until solid bony union is confirmed, usually around 3 months or longer.
Q4: Does this plate need to be removed?
A4: Because the hook plate is a specialized implant that spans the AC joint, most surgeons recommend a second surgery to remove it after the fracture has solidly healed (typically between 6 months to 1 year post-op). This is to optimize long-term shoulder function and avoid potential issues like subacromial impingement or bone erosion. This removal is a planned elective procedure.
Q5: How is the correct hook plate size selected for a patient?
A5: This decision is made by the surgeon based on precise pre-operative imaging (X-rays, CT scans). The surgeon will evaluate the size of the patient's clavicle, the fracture pattern, and the acromion anatomy to select the most appropriate model from the system's range of available sizes (e.g., hook length, plate length, number of holes) that best matches the individual's anatomy and provides optimal stability.

The Distal Radius Locking Plate is a high-precision internal fixation implant designed to treat distal radius fractures, offering stable support and promoting bone healing.
Details
The Olecranon Locking Plate is a high-strength internal fixation system designed for olecranon fractures, providing stable locking fixation to promote bone healing.
Details
The Ulna and Radius Locking Plate is made of high-strength titanium alloy, specifically designed for the treatment of wrist and forearm fractures, offering excellent stability and biocompatibility.
Details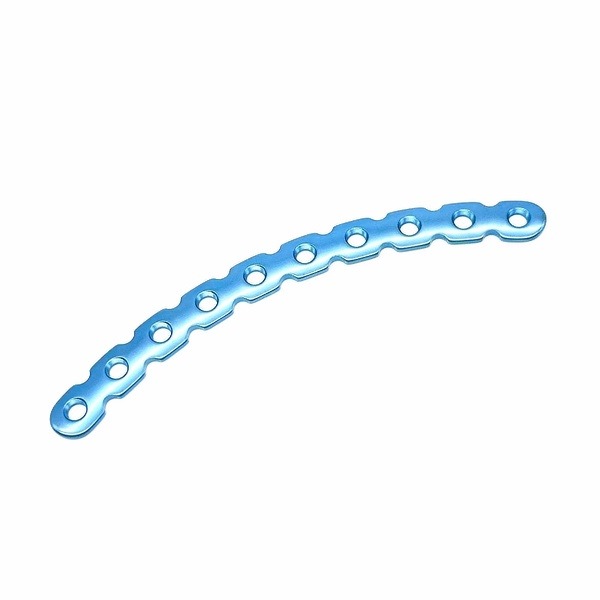
The Arc Reconstruction Locking Plate is a high-precision internal fixation implant designed for complex fracture repair, offering anatomically adapted curvature and stable locking fixation.
Details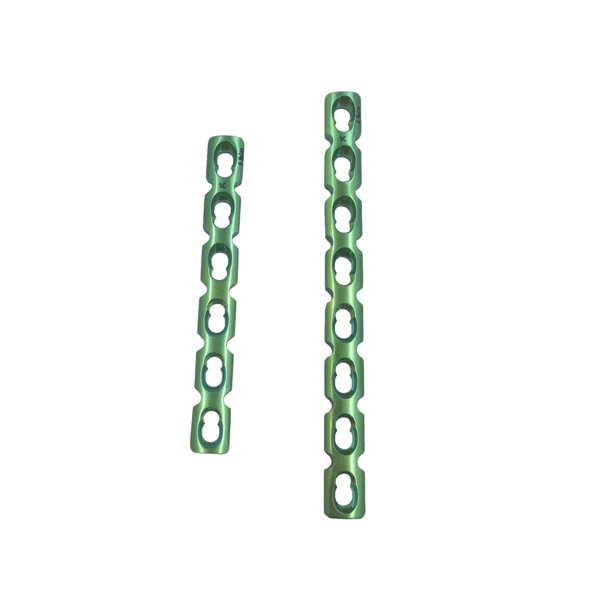
The reconstruction locking plate is designed for stable fixation of complex fractures, especially in anatomically challenging areas such as the clavicle and pelvis.
Details
Our medical grade U-type nail is the main medical instrument used for osteology procedures to fix fractures.
Details
Our titanium alloy traction cables are suitable for intramedullary fixation and bandaging of limb fractures.
Details
Our orthopedic metal bone pins are suitable for traction or internal fixation of limb fractures during fracture reduction.
Details
Sign up for our newsletter to get update information, promotion and insight.




 IPv6 network supported
IPv6 network supported






 Get A Quote
Get A Quote







